
Regulation of magnesium homeostasis and transport in mammalian cells
Magnesium is the fourth most abundant cation within the human body but the second within the cell after potassium. Under resting conditions, cellular magnesium ions (Mg2+) are abundantly compartmentalized within mitochondria, nucleus and endoplasmic or sarcoplasmic reticulum, with total concentrations ranging between 16 to 18 mM within each of these compartments. An additional significant pool of Mg2+ is found in the cytoplasm, where approximately 4 mM Mg2+ is bound to ATP and other phosphonucleotides. As a result of this cellular partitioning and buffering, free [Mg2+] in the cytoplasm or within the mitochondrial matrix has been estimated at 0.7-0.8 mM in most mammalian cells.
Cellular Mg2+ content is maintained below its electrochemical equilibrium by powerful transport mechanisms. Studies from our laboratory have identified the signaling mechanism responsible for the regulation of these entry and exit mechanism in cardiac and liver cells. Hormones such as epinephrine (adrenaline) and glucagon but also b-adrenergic stimulants (e.g. isoproterenol) enhance Mg2+ extrusion by activating a cAMP-phosphorylated Na+/Mg2+ exchanger. Conversely, hormones that counteract adrenoceptor stimulation (e.g. vasopressin or insulin) prevent Mg2+ extrusion and promote Mg2+ accumulation via PKCe signaling to TRPM7 and TRPM6 channels.
The long term interests of our research are: 1) to elucidate how Mg2+ transport and homeostasis are regulated, and 2) to understand the physiological consequences of changes in cellular Mg2+ content. Both these aspects of our research have major clinical relevance in that several diseases including diabetes, alcoholism, hypertension, asthma, and inflammation are characterized by a decrease in cellular and serum Mg2+ content. To address these questions, my laboratory uses a variety of biochemical, toxicological, and more recently molecular approaches and techniques. My laboratory also uses a variety of experimental models spanning from the whole animal to specific cells such as cardiac myocytes, liver cells, monocytes and macrophages, to subcellular components (e.g. plasma membranes, mitochondria, microsomal vesicles), to purified proteins.
Title
Legend
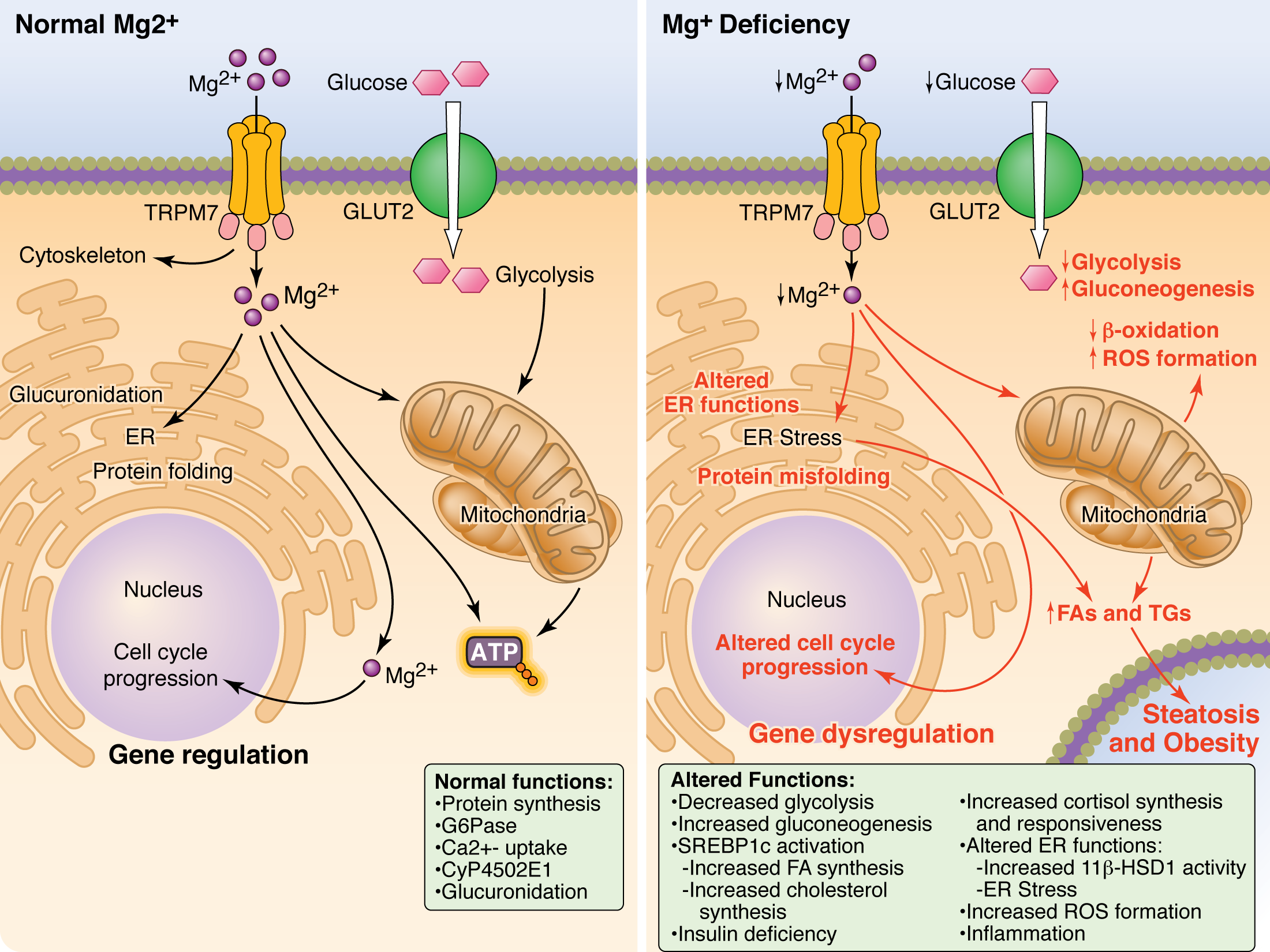
Role of Magnesium in liver and whole body metabolism
While studying Mg2+ transport in liver cells, we have observed a close association between Mg2+ extrusion and glucose output in liver cells. The hormones responsible for Mg2+ extrusion (catecholamine, glucagon, etc.) are the same hormones released by our body to maintain glucose homeostasis. The same is true for Mg2+ accumulation, as insulin promotes both glucose and Mg2+ accumulation within the liver.
We also observed that reducing dietary Mg2+ content or extracellular Mg2+ concentration in culture media resulted in a decreased accumulation and utilization of glucose within the hepatocyte. At the same time, PPARg and SREBP1c, two key regulators of fatty acid oxidation and metabolism were upregulated. These changes in liver metabolism are of major importance if we consider the current incidence of obesity in the US and the fact that the current Western diet provides about 35-40% less Mg2+ than physiologically required.
At the cellular level, Mg2+ deficiency has two distinct effects:
Role of Magnesium homeostasis in cell cycle regulation
Exposure to low extracellular Mg2+ reduces the cell reduplication rate. This has been observed in hepatocytes in culture and also in fibroblasts and cardiac myocytes. It is presently under investigation whether the slow-down in cell reduplication rate is the result of the energetic deficit described previously or whether magnesium deficiency affect the operation of specific genes and kinases (e.g. p21, p27 and p53) involved in the process.
These studies are of relevance to understand the role of magnesium in hepatocyte reduplication rate under physiological conditions as well as under pathological conditions such as alcoholism, hepatitis, cirrhosis, in which a high rate of hepatocyte cell death is observed. These studies may also lead to better understand unregulated cell growth (i.e. hepatic tumor and cancer)
Role of Magnesium in systemic and liver inflammation
Magnesium sulfate (MgSO4) is the therapy of choice for pathological conditions such as eclampsia (convulsion and hypertension during gestation) and pre-term labor. The effectiveness of MgSO4 has been attributed to its ability to inhibit Ca2+ entry through L-type Ca2+ channels in neurons and vascular endothelial cells (in eclampsia) and myometrium cells in pre-term labor. While there is merit in these assumptions, recent studies conducted in conjunction with Dr. Bernstein, an OB/GY physician at UH have evidence that MgSO4 greatly reduces synthesis and production of pro-inflammatory cytokine by inhibiting NF-kB signaling in monocytes of women undergoing pre-term labor. Importantly, pre-term newborns present a high incidence of cerebral palsy, which has been attributed to higher than normal levels of pro-inflammatory cytokines in the cerebral fluid.
We are continuing our studies with Dr. Bernstein to understand the short-and long-term implications of changes in cellular Mg2+ for the systemic response of immune-competent cells such as lymphocytes and dendritic cells. We are also expanding our study to the Kupffer cells, as these liver resident macrophages are involved in mediating the immune and inflammatory response in livers of animals and humans exposed to alcohol (ASH) and hepatitis.
| Diseases |
|---|
| Alcoholism, Diabetes, Obesity |
